Radiation for Breast Cancer: Protecting the Heart
The paper by Darby and others published March 14th 2013 in the New England Journal of Medicine has caused a firestorm of media coverage. The authors report on over 900 women who had been treated for breast cancer in Scandinavia who suffered a major coronary event and compared them with over twelve hundred control individuals. The Swedish women were treated between 1958 and 2001, the Danish women 1977 to 2000. The authors concluded that the risk of a major cardiac event increased by 7.4% for each incremental increase in mean cardiac dose of 1Gray (Gy). My concern as a breast surgeon is that these reports will dissuade women from receiving post-operative radiation for breast cancer, which has been proven to reduce recurrence rates.
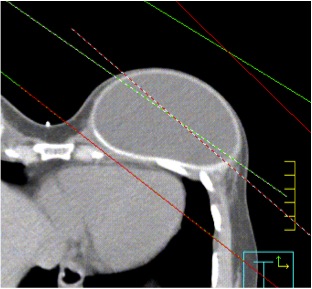
A portion of the heart is included in the radiated field with free-breathing radiation
I wish to extinguish some of these flames by emphasizing that we cannot extrapolate the results of antiquated treatment from a decade to over fifty years ago with the results that can be achieved with modern radiation techniques. The invisible high-energy beams of radiation therapy kill cancer cells by damaging their DNA. Radiation beams travel in straight lines, and cannot curve around concave structures. Careful treatment planning minimizes radiation to adjacent normal structures, which may otherwise also be damaged. Scatter of radiation to the heart, in particular the major coronary arteries, increases the risk of ischemic heart disease and heart attack. Radiation for left-sided breast cancers is more likely to cause adverse cardiac sequelae than treatment for right-sided cancer.
There have been considerable advances in the accuracy and targeting of radiation treatment, particularly with regard to heart-sparing techniques. According to Jaymeson Stroud MD, radiation oncologist with Mercy Hospital St. Louis, “Radiation techniques have advanced considerably in the last sixty years. In the 1950s low energy linear accelerators and Cobalt 60 were used. Computerized two-dimensional treatment planning using port field X rays and use of treatment simulators did not come into being till the mid 60s.” He adds, “CT three dimensional planning was introduced in the 1980s, and even more tailored techniques such as intensity modulated radiation therapy (IMRT) a decade later.” IMRT utilizes high-energy beamlets to “curve” the dose to avoid normal structures and thus diminish incidental exposure to the heart. The patients in the Scandinavian study received their therapy before the era of three-dimensional CT treatment planning.
All of the patients in the NEJM paper received external beam radiation. Twenty two percent had breast-conserving surgery and the remainder underwent mastectomy. Accelerated partial breast irradiation (which treats a well localized rim of tissue centered on the tumor bed), can reduce doses to surrounding normal structures depending on the location of the tumor in the breast. APBI can be achieved using external beam techniques, or placing the radiation source within the breast (brachytherapy). Balloon catheter techniques such as Mammosite®, Contura® and Savi® are all designed to concentrate the site of radiation.
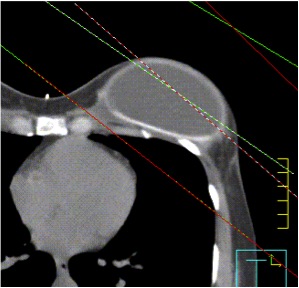
With deep breath hold techniques the heart is no longer in the radiation field
Targeted intraoperative radiation therapy (IORT) for breast cancer has been under study since 2000. A single dose of radiation is delivered to the lumpectomy bed while the patient is still on the operating table. The results of the international TARGIT-A trial were published in the Lancet in 2010 and revealed that local recurrence rates were equivalent to external beam RT. Updated data on almost 3500 patients were presented in San Antonio in December 2012; patients in the IORT group had fewer non-breast cancer deaths with a trend towards less mortality.
Kathy Baglan MD, a radiation oncologist, adds that modern external beam heart-sparing techniques such as the Active Breathing Coordinator— which separates the heart from the chest wall during deep breath holds— and treating the patient on the prone rather than supine position, can ensure that no heart is caught in the crossfire of the radiation beam. Please see the attached images showing the heart moving away from the radiation beam during inspiration. These are extra efforts on the part of the savvy radiation oncologist that are not reimbursable. She states, “Not only has radiation been shown to decrease local recurrence rates, but a very large study from Duke University of 112,000 women treated with more modern RT between 1990 and 2004 showed that compared to mastectomy, patients undergoing lumpectomy and breast radiation were fourteen percent less likely to die of breast cancer and nineteen percent less likely to die of any cause. This clearly shows that “good” radiation saves lives, not shorten lives.”
She adds, in reference to the paper by Darby et. al., “To put the Scandinavian results in perspective, for a 50 year-old woman with no preexisting cardiac risk factors, a mean heart dose of 3 Gy (which is high for today’s standards) would increase her absolute risk of dying from ischemic heart disease by age 80 from 1.9% to 2.4% (i.e. 0.5%) and increase her risk of having any major cardiac event from 4.5% to 5.4% (0.9% difference).
As physicians we are all aware that our treatments can cause harm. Every effort has to be made to reduce harm. The authors of the NEJM paper conclude that clinicians have to consider cardiac dose and cardiac risk factors when making decisions about the use of radiation therapy. I suggest that the issue is not whether radiation should be used at all, but whether the radiologist will tailor, customize and individualize the treatment to spare the heart. Patients should discuss with their radiation oncologist what heart-sparing approaches would benefit them.
Images courtesy of Dr. Stroud.
Tags: Active Breathing Coordinator, brachytherapy, breast cancer, breast cancer treatment, breast conservation therapy, Contura, heart-sparing radiation, IMRT, IORT, Mammosite, post-mastectomy radiation, prone radiation, radiation, Savi, TARGIT-A trial